Screening
- Applied at the population level among asymptomatic individuals.
- Screening should only be done if there are effective interventions among presymptomatic individuals. Else it may be worth waiting for symptoms.
- An individual who does not actually have the disease but is predicted to have it will be enrolled into the healthcare system unnecessarily.
- Disease prevalence should be expected to be much lower than in diagnostic settings - remember issues with PPV from Demonstration 1.
- If screening has any side effects, than many individuals may be exposed to them.
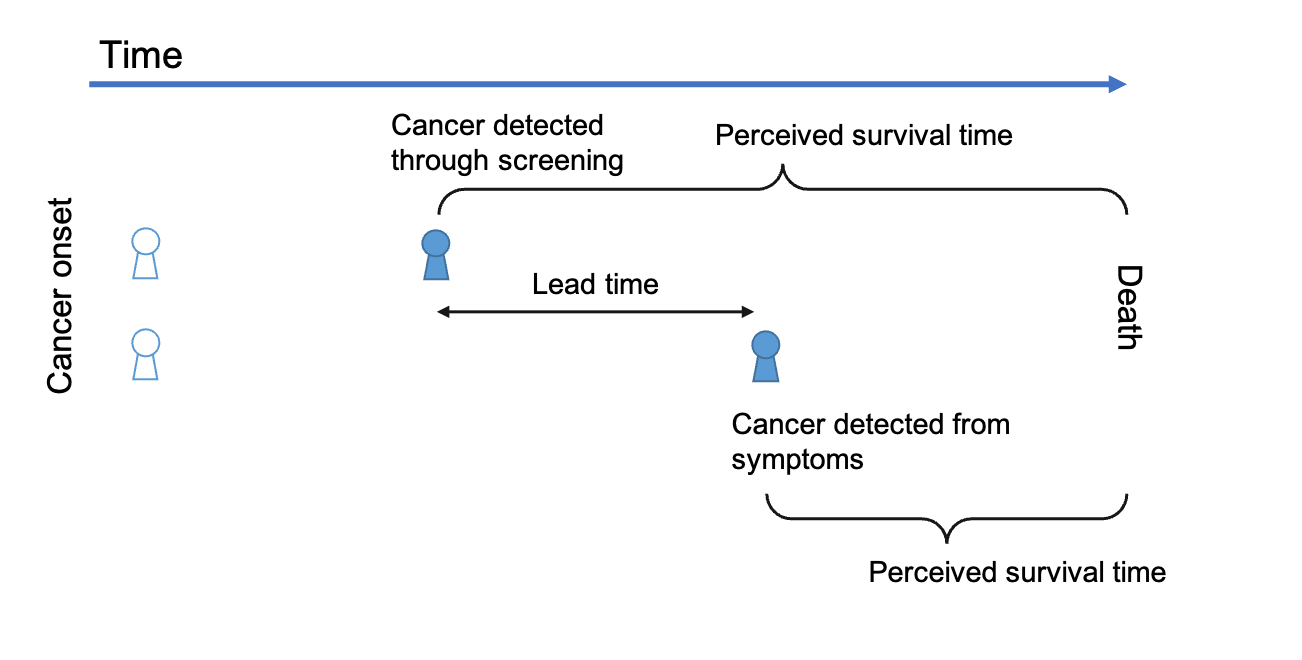
Lead-time bias
- Screening leads to early detection - early detection does not have any benefit.
- Two patients die at the same time, but one was screened and cancer detected earlier.
- The first individual is followed for longer.
- Lead time bias: when length of follow-up makes you conclude that screening is useful: "Individuals lived longer due to screening".
- Lead time bias: when you attribute benefit to simply observing people.
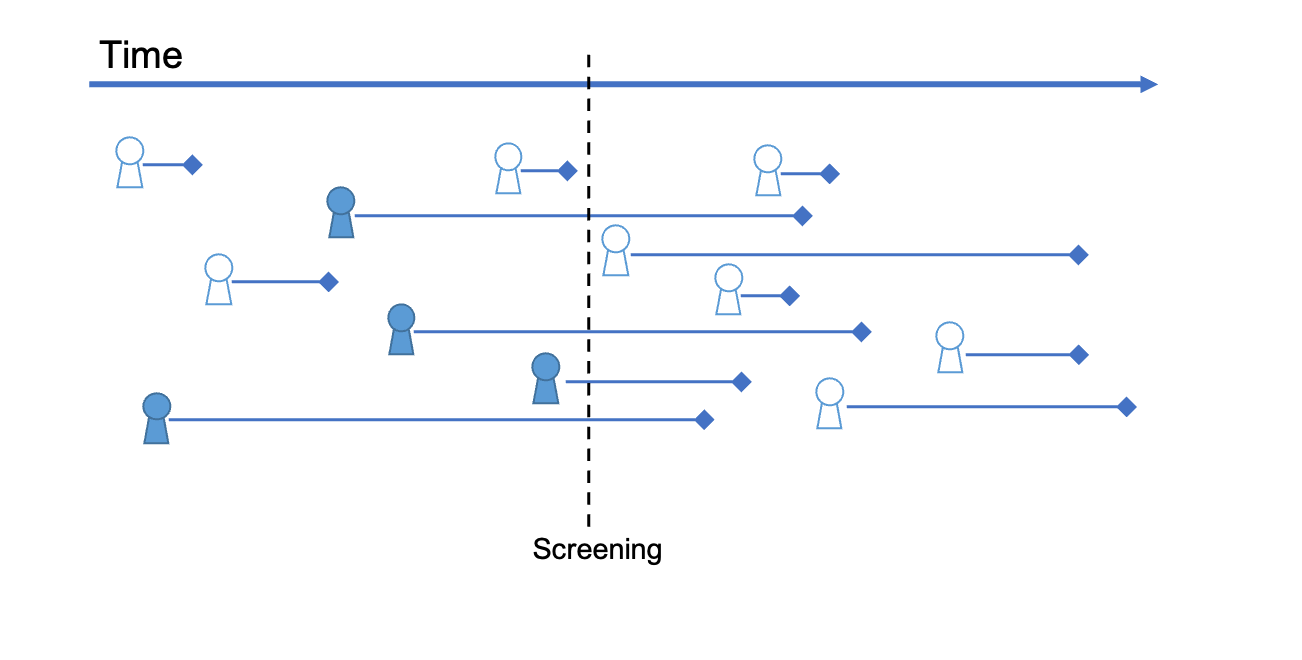
Length-time bias
- Same number of fast and slow growing tumors over a period of time.
- By chance, screening will find more slow growing tumors.
- People with fast growing cancers will be diagnosed once symptoms are detected (or postmortem).
- Length time bias: concluding that screening has an effect on cancer progress and risk of death when in fact slower growing cancers are oversampled by screening.
No gold standard
- Predicitive assessments requires us to know the true value (Y+ or Y-).
- If no gold standard exists which is efficient in classifying individuals then this adds further uncertainty to our estimates.
Missing data and selection bias
- Predictions based on data for which there is systematic missingness - findings are biased.
- Cannot generalise as easily, since datapoints collected are not from a random sample.
- If we continuously screen, but the screening oversamples individuals with high risk, then we create a selection bias and PPV may be inflated.
Measurement bias
- Even with a perfectly random sample from the correct population we may still be measuring the wrong thing.
- Different measurement methods results in different Y+ and Y- classifications, biasing the estimate of prevalence.
- Not always a problem (!) - The link between cancer and smoking is not dependent on the person reporting smoking 20 or 25 cigarettes per day.
- Smoking cessation interventions targeting "smokers" may be helpful regardless of the exact number of cigarettes smoked.