Stability of criteria
- Revision of definitions, for instance risky drinkers.
- New protocols/questionnaires for screening.
- Technological advancements and new biomarkers.
- Local or cultural differences.
- Political leadership and incentives.
- ICD definitions change (The International Classification of Diseases, Injuries, and Causes of Death).

What is the actual prevalence when definitions/criteria change?
Alcohol screening
CAGE
- C: Have you felt the need to cut down your drinking?
- A: Have you ever felt annoyed by someone criticizing your drinking?
- G: Have you ever felt bad or guility about your drinking?
- E: Have you ever had an eye-opener - a drink the first thing in the morning to steady your nerves?
Responding Yes to one or more of the questions denotes a need for further assessment.
AUDIT-C
- How often do you have a drink containing alcohol? Never; Monthly or less often; 2 to 4 times a month; 2 to 3 times a week; 4 or more times a week.
- How many standard drinks containing alcohol do you have on a typical day when you are drinking? One or two; Three or four; Five or six; Seven to nine; 10 or more.
- How often do you have six or more drinks on one occasion? Never; Less than monthly; Monthly; Weekly; Daily or almost daily.
Scoring is 0 for never, and 1, 2, 3, or 4 for the subsequent answer choices in each question. The cut-off score for the AUDIT-C is usually a total of 3 points for women and 4 for men: ie, a score of 3 or higher for women and a score of 4 or higher for men indicate alcohol use disorder and the need for further assessment.
Different criteria for men and women in AUDIT-C, not so for CAGE - based on perception in CAGE based on consumption in AUDIT-C.
Risky drinking in Sweden
- CAN (Centrum för alkohol och narkotika)
- More than 9/14 (female/male) drinks per week or at least once a month an episode of heavy drinking (> 3/4 (female/male)).
- Risky drinking: 22% (female) and 38% (male)
- Public Health Agency of Sweden (Folkhälsomyndigheten)
- AUDIT-C
- Risky drinking: 13% (female) and 20% (male)
What is the actual prevalence when definitions/criteria are different?
Missing/Selective data
We rarely (if ever) have the entire population of interest in our cohort, but we often (almost always) want to infer something about the population. Those data points that are missing may bias our results.
- Would the measured prevalence be the same if we included everyone?
- Are some individuals, defined by some characteristic, more/less likely to be part of our cohort?
- Is the cohort sampled from the population which we want to infer something about?
- Are you trying to generalise to the same definition of the population from which the cohort was sampled? For instance: all university students vs. program students vs. students taking single courses.
Recommended reading
Selection bias (Catalogue of Bias)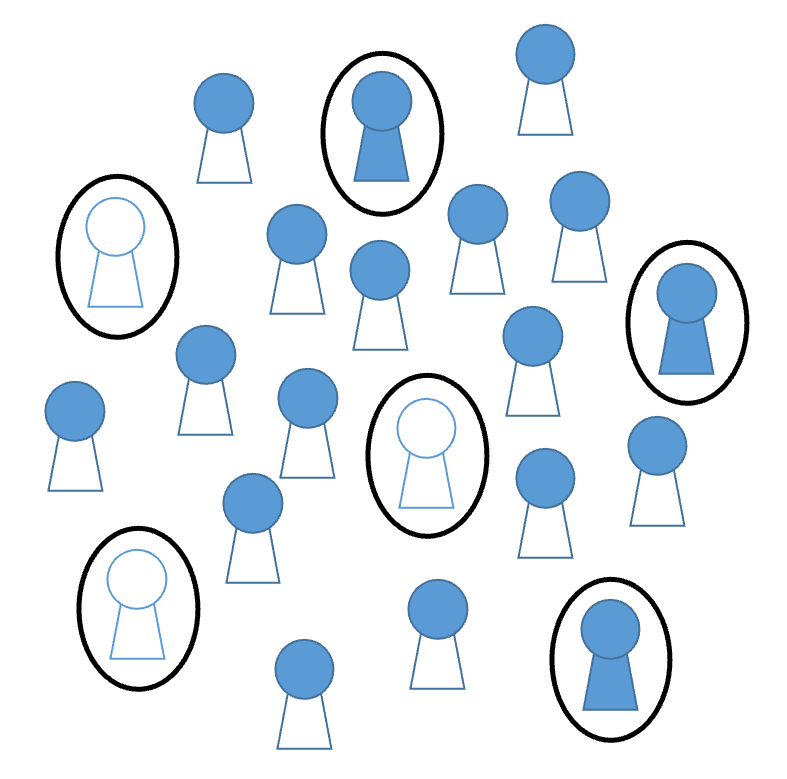
Defining a case
When we talk about cases, we make the assumption that people can be placed in either the affected or non-affected category. This is often a very useful assumption, but can be misleading. Naturally there is a difference between those who have been exposed to asbestos once every day versus those who have been exposed once every month.
But it is often not the precise measurement of a phenomena that is important in epidemiology (in contrast to in physics where it is very important), but rather it is important to have a measurement that can help us make people more healthy.
A case or affected may be defined in several ways when a dichotomy is not natural:
- Statistical cutoffs - Two standard deviations away from the (conditional) mean, ie. abnormal values are considered cases.
- Clinically relevant cutoffs - Risky drinkers are at higher risk of negative consequences.
- Prognostic value - Values below a threshold does not help us make a prognosis for the patient.
- Operational - Rule of thumb which helps us identify people at risk, eg. BMI cutoffs, which are easy to remember. Does not mean that people below the cutoff are without risk.
